Get Maine Advance Template in PDF
Similar forms
The Maine Advance Directive form shares similarities with the Durable Power of Attorney (DPOA) for Health Care. Like the Maine form, a DPOA allows individuals to appoint someone they trust to make health care decisions on their behalf when they are unable to do so. Both documents empower the chosen agent to make critical medical choices, including treatment options and end-of-life care. The DPOA also emphasizes the importance of the agent understanding the individual's values and preferences, similar to how the Maine Advance Directive outlines the agent's responsibilities in making decisions consistent with the principal's wishes.
Another comparable document is the Living Will. This legal document outlines an individual's preferences for medical treatment in situations where they are unable to communicate their wishes. The Living Will specifically addresses end-of-life care and the types of medical interventions one would or would not want. Much like the Maine Advance Directive, it serves to guide health care providers and loved ones in making decisions that align with the individual's values. Both documents aim to ensure that a person's wishes regarding medical care are respected, even when they cannot express them directly.
The Health Care Proxy is also similar to the Maine Advance Directive. This document allows a person to designate an agent to make health care decisions for them in the event they become incapacitated. Like the Maine form, the Health Care Proxy requires that the designated agent act in the best interest of the individual, following their expressed wishes. Both documents emphasize the importance of communication about health care preferences and the need for the agent to have access to the individual's medical information to make informed decisions.
For those interested in property transactions, the Ohio form for a Quitclaim Deed is a vital document, providing a structured way to transfer property interests without the need for extensive guarantees. Understanding its practical applications can make a significant difference; for more information, you can explore a helpful resource on how a Quitclaim Deed can facilitate this process when dealing with property transfers.
Finally, the Do Not Resuscitate (DNR) order is another document that aligns with the Maine Advance Directive. A DNR specifically instructs medical personnel not to perform cardiopulmonary resuscitation (CPR) if the individual's heart or breathing stops. While the Maine Advance Directive encompasses a broader range of health care decisions, the DNR serves as a specific directive regarding resuscitation efforts. Both documents reflect an individual’s choices about medical care and are crucial for ensuring that their wishes are followed during critical health situations.
Misconceptions
- Misconception 1: The Maine Advance form is only for people who are terminally ill.
- Misconception 2: You must fill out the entire form to make it valid.
- Misconception 3: Your agent can make any decision they want, regardless of your wishes.
- Misconception 4: Once the form is signed, you cannot make any changes.
- Misconception 5: The form is not legally binding.
This form is not limited to those with terminal illnesses. It is designed for anyone who wants to outline their health care preferences in case they become unable to communicate those wishes in the future.
You can choose to complete only specific parts of the form. Completing any part is sufficient to express your wishes, as long as you sign and date it in Part 6.
Your agent must follow your stated wishes if you have provided them in the form. If you have not specified your wishes, your agent should make decisions based on your values or best interests.
You can change any part of the form, except for Parts 6 and 7. If you make changes, it is advisable to initial and date each modification to show it was your decision.
The Maine Advance form is legally binding once it is properly signed and witnessed. It serves as an official document that communicates your health care preferences to your medical providers and family.
Popular PDF Documents
Afppgmc Updating Online - Each section of the form is intended to gather comprehensive information about the applicant.
The California Notice to Quit form is crucial for landlords aiming to begin the eviction process, as it clearly communicates the reasons for eviction and the timeline for tenants to respond. For more information and access to an editable version of this important document, landlords can visit https://californiapdf.com/editable-notice-to-quit/.
Maine Dmv - The physician must provide their name, signature, and license number on the form.
What Is a Sales Contract - The deed transfer will be free from significant encumbrances, preserving the property's utility for the Buyer.
Documents used along the form
The Maine Advance Directive form serves as an essential tool for individuals to communicate their health care preferences. Along with this form, several other documents may be utilized to ensure comprehensive planning for medical care and end-of-life decisions. Below is a list of additional forms and documents that are commonly used in conjunction with the Maine Advance Directive.
- Durable Power of Attorney (DPOA): This document allows an individual to appoint someone to make financial decisions on their behalf if they become incapacitated. It is crucial for managing financial affairs during periods of illness.
- Do Not Resuscitate (DNR) Order: This order communicates a patient's wish not to receive cardiopulmonary resuscitation (CPR) in the event of cardiac or respiratory arrest. It must be signed by a physician and the patient or their agent.
- Living Will: A living will outlines specific medical treatments an individual wishes to receive or avoid in case they are unable to communicate their preferences. It provides guidance to health care providers and family members.
- Organ Donation Form: This form allows individuals to specify their wishes regarding organ and tissue donation after death. It can be included as part of the Advance Directive or as a standalone document.
- Health Care Proxy Form: This document designates a person to make health care decisions on behalf of another individual. It is similar to the agent designation in the Advance Directive but may be used separately.
- HIPAA Release Form: This form authorizes the release of medical information to designated individuals, ensuring that family members or agents can access necessary health information when making decisions.
- Employee Handbook Form: This crucial document outlines important company policies and expectations for employees. To ensure you have all necessary information, consult the PDF Templates for further guidance.
- Funeral Planning Document: This document outlines an individual's preferences for funeral arrangements and burial decisions. It can ease the burden on family members during a difficult time.
- Guardian Nomination Form: This form allows individuals to nominate a person to be appointed as their guardian should they become unable to make decisions about their personal care. It provides clarity on who they trust to make such decisions.
Utilizing these documents in conjunction with the Maine Advance Directive can create a comprehensive plan for health care and personal preferences. It is advisable to discuss these documents with family members, health care providers, and legal advisors to ensure that all wishes are understood and respected.
Form Preview Example
Maine Health Care
Advance Directive Form
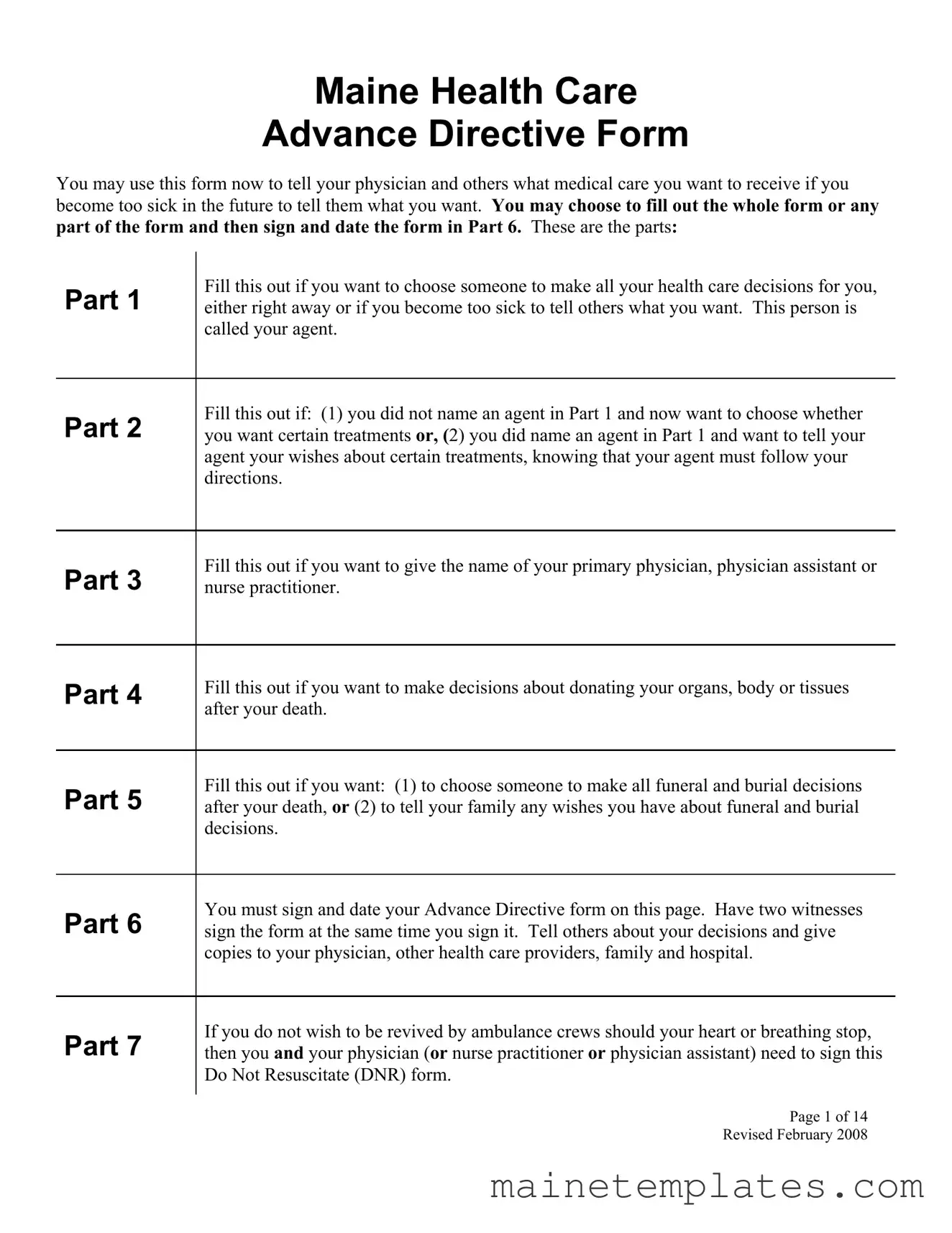
You may use this form now to tell your physician and others what medical care you want to receive if you become too sick in the future to tell them what you want. You may choose to fill out the whole form or any part of the form and then sign and date the form in Part 6. These are the parts:
Part 1 |
Fill this out if you want to choose someone to make all your health care decisions for you, |
either right away or if you become too sick to tell others what you want. This person is |
|
|
called your agent. |
Part 2 |
Fill this out if: (1) you did not name an agent in Part 1 and now want to choose whether |
you want certain treatments or, (2) you did name an agent in Part 1 and want to tell your |
|
|
agent your wishes about certain treatments, knowing that your agent must follow your |
|
directions. |
Part 3 |
Fill this out if you want to give the name of your primary physician, physician assistant or |
nurse practitioner. |
Part 4 |
Fill this out if you want to make decisions about donating your organs, body or tissues |
|
after your death. |
||
|
Part 5 |
Fill this out if you want: (1) to choose someone to make all funeral and burial decisions |
after your death, or (2) to tell your family any wishes you have about funeral and burial |
|
|
decisions. |
Part 6 |
You must sign and date your Advance Directive form on this page. Have two witnesses |
sign the form at the same time you sign it. Tell others about your decisions and give |
|
|
copies to your physician, other health care providers, family and hospital. |
Part 7 |
If you do not wish to be revived by ambulance crews should your heart or breathing stop, |
then you and your physician (or nurse practitioner or physician assistant) need to sign this |
|
|
Do Not Resuscitate (DNR) form. |
Page 1 of 14 Revised February 2008
Note
You may change any part of this form except for Part 6 and Part 7. You may cross out any words, sentences, or paragraphs you do not want. You can also add your own words. If you make any changes to the form, it is best if you put your initials and the date next to each change so that everyone knows it was your decision to make the change. The form lets you choose different ways to handle your care by checking boxes or filling in blanks. You may initial each box and each blank you fill in to show that it was your decision to check the box or fill in the blank.
Before filling out this form, we suggest that you talk with your lawyer, family members, physicians, and others close to you about your wishes. If you make changes or complete a new form, be sure to let everyone know.
My Name (please print)______________________________________________________
My Address _______________________________________________________________
My Birth date______________________________________________________________
This is a list of all the people who have copies of my signed health care advance directive:
1. ________________________________________________________________________
2.________________________________________________________________________
3.________________________________________________________________________
4. ________________________________________________________________________
5. ________________________________________________________________________
6. ________________________________________________________________________
7. ________________________________________________________________________
8. ________________________________________________________________________
9. ________________________________________________________________________
10. ________________________________________________________________________
Page 2 of 14
Revised February 2008
Part 1 – Power of Attorney for Health Care
Instructions:
This part lets you choose another person to make health care decisions for you, either right away or when you are too sick to choose your own care. The person you choose is called your agent. You may also name a second and third choice to be your agent, if your first choice is not willing, reasonably available or able to make decisions for you. If you choose an agent on this form, but do not fill out any other parts of the form, your agent will be able to:
•Make all health care decisions for you, including decisions regarding tests, surgery and medication;
•Decide whether or not to have food or fluids given to you through tubes or fed into your veins through an IV;
•Decide whether or not to use treatments or machines to keep you alive or to restart your heart or breathing;
•Choose who will give you health care and where you will get it, such as hospitals, nursing homes, assisted living settings, home health, or hospice care; and
•Make any health decision he or she believes would be consistent with your values or in your best interest, even if it is not listed in the form.
Who can be your agent:
You can name any adult you trust to be your agent, except your agent may not be the owner, operator or employee of a nursing home or residential
How your agent must make decisions:
If your agent does not know what you want, the agent must make decisions consistent with your personal values, if known, or based on your best interests. In Part 2, you can decide what you want in advance. If you make choices in Part 2, your agent must make decisions based on those choices.
Who can see your health care information:
Once your agent has the right to make health care decisions for you, your agent can look at your medical records and consent to giving your medical information to others. The state and federal privacy laws let your agent see all of your health information so that he or she can make the right decision for you.
The first part of your advance directive begins on the next page.
Page 3 of 14 Revised February 2008
YOUR ADVANCE DIRECTIVE BEGINS HERE
Choosing an agent: Fill in your name and the name of the person you choose to be your agent to make health care decisions for you here:
My name______________________________________________________________________________
My agent’s name________________________________________________________________________
Title or relationship to me_________________________________________________________________
My agent’s address______________________________________________________________________
My agent’s home phone (___)___________________ My agent’s work phone (___)__________________
If the agent I have named above is not willing, reasonably available or able to make decisions for me, I choose the following person to be my agent:
If the person I have named as Choice # 2 is not willing, reasonably available or able to make decisions for me, I choose the following person to be my agent:
Choice # 2 to be my agent |
Choice # 3 to be my agent |
|
Name____________________________________ |
Name_________________________________ |
|
Title or Relationship to me___________________ |
Title or Relationship to me________________ |
|
Address__________________________________ |
Address_______________________________ |
|
_________________________________________ |
______________________________________ |
|
Home Phone (___)__________________________ |
Home Phone (___)_______________________ |
|
Work Phone (___)__________________________ |
Work Phone (___)_______________________ |
|
You may change your mind later about who you want to be your agent. If you want to stop the agent you have named from making decisions for you, you must tell your primary physician or fill in these blanks:
I do not want ________________________ to be my agent. _______________________________________
My signature
Date you filled out and signed this section _________________________
Any time you cancel, replace or change this form you should give copies of the changed or new form to everyone who has a copy of your original form.
Page 4 of 14
Revised February 2008
Your agent’s power:
When your agent can start making decisions for you: (Check only one box: A or B)
A. My agent can make decisions only when my primary physician or a judge decides that I am too sick to make my own health care decisions.
OR
B. My agent can start making health care decisions for me right away, but this does not mean I have given up the right to make my own decisions if I am still able and willing to make my own decisions. When my agent makes a health care decision for me, I will be told, if possible, about that decision before it is carried out unless I say I do not want to know. If I disagree with that decision and am still able to decide, I can make a different decision. As long as I am able, I can end my agent’s right to make decisions for me, change my agent or make my own decisions. If I want to end my agent’s right to make decisions for me, I must tell my primary physician or put my decision in writing and sign it with the date of my signature.
Nominating a guardian:
A guardian is a person chosen by a court to make decisions about your personal care. These decisions can include not only health care, but other decisions such as where you will live and how your personal needs will be met. If you wish, you may ask that a court assign your agent as your guardian, if appointment of a guardian should become necessary. Check the box below to nominate your agent to be your guardian, if a judge needs to appoint a guardian for you.
I nominate my agent to be my guardian if a judge needs to appoint a guardian for me.
If you want to nominate someone other than your agent to be your guardian, you may fill in the section below.
If a judge needs to appoint a guardian for me, I nominate the person named below as my guardian:
Name__________________________________________ Title or Relationship to me________________
Address______________________________________________________________________________
_____________________________________________________________________________________
Home Phone (___)_______________________ Work Phone (___)______________________________
Page 5 of 14 Revised February 2008
Part 2 – Special Instructions
Instructions if you did not name an agent in Part 1:
If you did not name an agent in Part 1, you should fill out this Part to state what you want for care if you become too sick to make your choices known.
OR
Instructions if you did name an agent in Part 1:
If you named an agent in Part 1, you do not have to fill out this part of the form. If you want your agent to make all of your health care decisions, DO NOT fill out this part of the form. Your agent will make decisions in your best interests, including decisions to refuse treatment. However, you may fill out this part if you want to give special directions to your agent about your wishes, such as when you are near death, in a permanent coma or no longer able to make your own decisions. You may also cross out or add words. It is best if you put your initials and date next to any changes you make so everyone knows the changes were your decision. If you complete this part, your physician and others will follow these instructions and your agent cannot make a different decision. You may also write your wishes on another piece of paper, sign it, date it, and keep it with this form.
You may check one of the two boxes below to show your choice about getting treatments that would keep you alive:
Choice not to be kept alive |
Choice to be kept alive |
|
I do not want treatment to keep me alive if my |
I want to be kept alive as long as possible |
|
physician decides that either of the following is true; |
within the limits of generally accepted health |
|
(i) I have an illness that will not get better, cannot |
care standards, even if my condition is |
|
terminal or I am in a persistent vegetative |
||
be cured, and will result in my death quite soon |
||
state. |
||
(sometimes referred to as a terminal condition), |
||
|
||
OR |
|
|
(ii) I am no longer aware (unconscious) and it is very |
|
|
likely that I will never be conscious again (sometimes |
|
|
referred to as a persistent vegetative state). |
|
|
|
|
Page 6 of 14
Revised February 2008
You may also check one of the two boxes below to show your choice about treatment that would keep you alive if, in the future, you have late stage Alzheimer’s disease or other severe dementia. These choices will not limit the authority under state law for your agent, surrogate, guardian or physician to make treatment choices if you are unable to make your own decisions and are not in late stage Alzheimer’s disease or other severe dementia.
Choice not to be kept alive
If my physician and a second physician decide that I am in the late stage of Alzheimer’s disease* or other severe dementia, I do not want treatment to keep me alive.
Choice to be kept alive
I want treatment to keep me alive as long as possible within the limits of generally accepted health care standards, even if my physician and a second physician decide that I am in the late stage of Alzheimer’s disease or other severe dementia.
*Only a physician can determine that someone is in the late stage of Alzheimer’s disease. People in the late stages of Alzheimer’s disease generally have a number of the following characteristics: loss of the ability to respond to their environment; loss of the ability to speak; loss of the ability to control movement; loss of the capacity for recognizable speech, although words or phrases may occasionally be uttered; needing help with eating and toileting; general incontinence of urine; loss of the ability to walk without assistance, then the ability to sit without support, then the ability to smile, and the ability to hold their head up; reflexes become abnormal; muscles grow rigid; and swallowing is impaired.
Tube Feeding: You may check one of the two boxes below to show your choice about tube feeding or having water and nutrition fed into your body through an IV or tube (artificial nutrition and hydration):
Artificial nutrition and hydration should not be given, or should be stopped, based on the other
Artificial nutrition and hydration should be given regardless of my condition.
Page 7 of 14 Revised February 2008
Relief from Pain: You may check the box or fill in the blanks below to show your choice about relief of pain or discomfort.
I want treatment for relief of pain or discomfort to be given at all times, even if it shortens the time until my death or makes me drowsy, unconscious or unable to do other things.
These are my wishes about relief of pain or discomfort:
Other Directions:
You may give more directions or add any other treatment choices in the space below:
Page 8 of 14 Revised February 2008
Part 3 — Primary Physician
This section is optional. Fill out this part only if you wish to name your primary physician today.
Name of my primary physician:__________________________________________________________
Address: _____________________________________________ Phone: ________________________
I want any agent I named in Part 1 to talk with this physician about my health care. If the physician I have named above is not willing, reasonably available or able to carry out my wishes, I want the agent I named in Part 1 to talk with the physician listed below:
Name of physician: _____________________________________________________________
Address:_____________________________________________ Phone:___________________
If you want your agent or those making decisions for you to speak with a nurse practitioner or physician assistant before making a decision, you may complete the following section:
Name of nurse practitioner or physician assistant: _____________________________________
Address: _____________________________________________ Phone:___________________
Page 9 of 14 Revised February 2008
Part 4 – Donation of Body,
Organs or Tissues at Death
This section is optional. Fill out this part only if you want to give directions about donating your body, organs or tissues after your death.
I do NOT wish to donate any organs, tissues or parts.
I have checked below my choices about donating my body, organs or tissues after death. I have spoken with my family so that they will not object to my wishes after I die.
I give my body. OR
I give any needed organs, tissues or parts. OR
I give only the following organs, tissues, or parts:
____________________________________________________________________
____________________________________________________________________
My gift is for the following purposes (you may check any number of boxes):
My gift is for transplant or therapy for another person, to be chosen based on generally accepted health care standards.
My gift is for research and education. My preference, if any, is to give my body, organs, or tissues to the following hospital, medical school, or physician:
Name ________________________________________________________
Address _______________________________________________________
________________________________________________________
I understand that I may need to contact the hospital, medical school, or physician before I die in order for them to accept my body, organs or tissues after my death.
Page 10 of 14 Revised February 2008
File Attributes
| Fact Name | Fact Description |
|---|---|
| Purpose | The Maine Health Care Advance Directive Form allows individuals to express their medical care preferences in case they become unable to communicate those wishes in the future. |
| Agent Designation | In Part 1, individuals can appoint an agent to make health care decisions on their behalf, either immediately or when they can no longer make decisions themselves. |
| Treatment Preferences | Part 2 provides a section for individuals to outline specific treatment preferences, which their appointed agent must follow if decisions need to be made. |
| Primary Physician | Part 3 allows individuals to designate their primary physician, physician assistant, or nurse practitioner for reference in their advance directive. |
| Organ Donation | Individuals can express their wishes regarding organ, body, or tissue donation in Part 4 of the form. |
| Funeral Decisions | Part 5 enables individuals to appoint someone to make funeral and burial decisions or to communicate their wishes regarding these matters to their family. |
| Signature Requirement | Part 6 requires individuals to sign and date the form, along with having two witnesses sign at the same time, to validate the directive. |
| Do Not Resuscitate (DNR) | Part 7 includes a DNR option, allowing individuals to specify that they do not wish to be revived by ambulance crews if their heart or breathing stops. |
Detailed Guide for Using Maine Advance
Filling out the Maine Advance form is a straightforward process that allows you to express your healthcare wishes clearly. Once you have completed the form, it’s essential to share your decisions with your healthcare providers and loved ones to ensure everyone is informed about your preferences.
- Gather Your Information: Before starting, collect your personal details, including your name, address, and birth date.
- Choose Your Agent: In Part 1, write the name of the person you want to make healthcare decisions for you. You can also name a second and third choice in case your first choice is unavailable.
- Specify Your Agent's Authority: Indicate when your agent can start making decisions for you by checking either box A (only when you are unable) or box B (immediately, while you are still able).
- Provide Your Agent’s Contact Information: Fill in your agent’s address and phone numbers for both home and work.
- Consider Nominating a Guardian: If you want your agent to be your guardian in case one is needed, check the appropriate box. You can also nominate someone else if desired.
- Fill Out Additional Parts: If you wish to specify treatment preferences, provide your primary physician’s name, or make organ donation decisions, complete Parts 2, 3, and 4 as applicable.
- Funeral and Burial Wishes: In Part 5, outline any wishes you have regarding funeral and burial decisions or designate someone to handle these matters for you.
- Sign and Date the Form: Go to Part 6 to sign and date the form. Ensure that two witnesses sign the form at the same time.
- Distribute Copies: After signing, share copies of the completed form with your physician, healthcare providers, family members, and anyone else involved in your care.
- Review and Update as Necessary: Keep in mind that you can change any part of the form except for Parts 6 and 7. If you make changes, initial and date them for clarity.